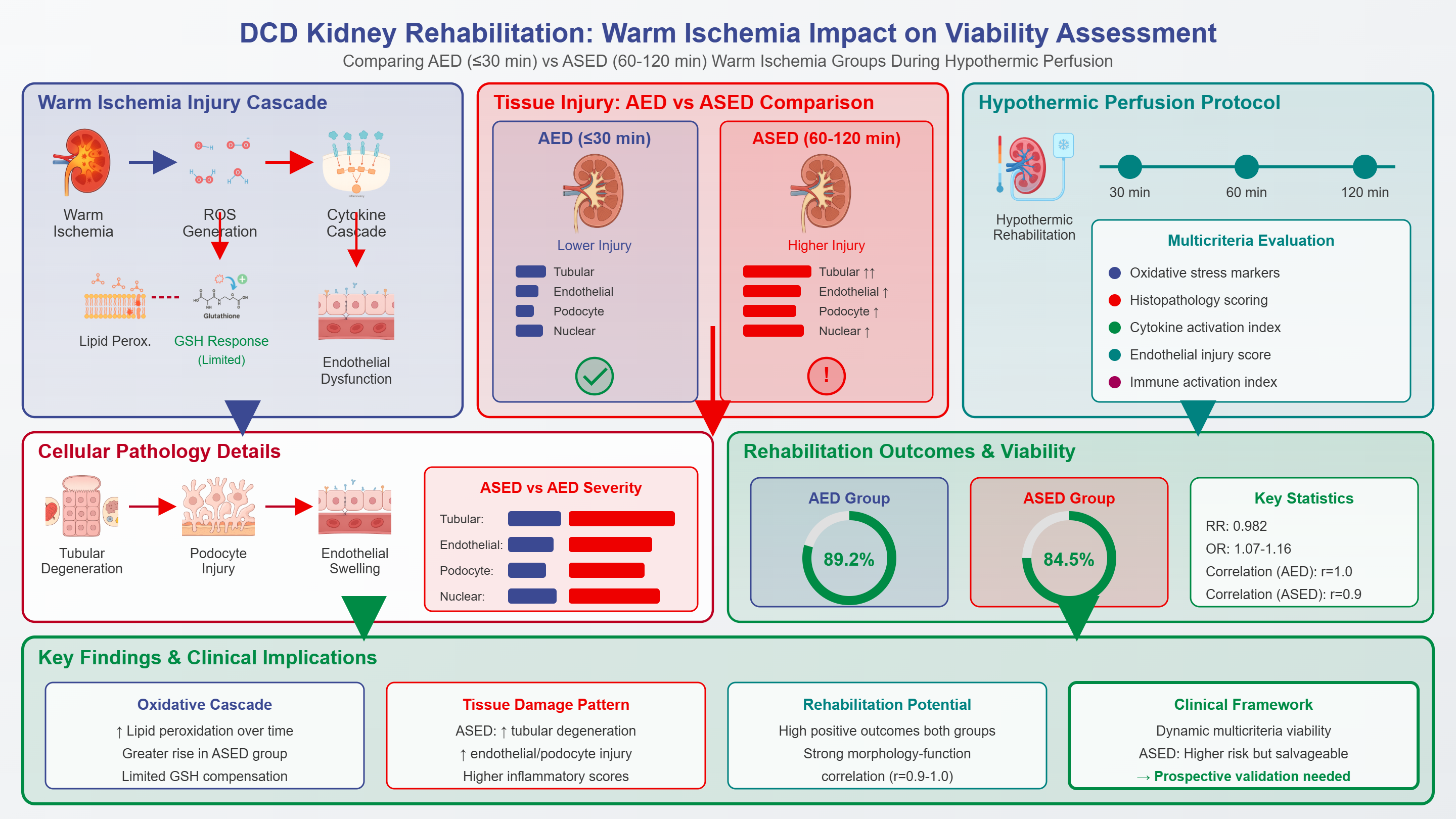
Global organ shortages have intensified interest in donation after circulatory death (DCD). However, DCD kidneys are affected by warm ischemia, which amplifies ischemia-reperfusion injury via a reactive oxygen species-damage-associated molecular pattern-cytokine-endothelial cascade, increasing the risk of microvascular dysfunction and delayed graft function. This study developed an objective postmortem ex vivo model to compare asystolic early donors/rapid death (AED; warm ischemia ≤30 min) and asystolic extended/delayed donors (ASED; 60–120 min) using integrated morphofunctional, biochemical, and immuno-inflammatory indicators during hypothermic perfusion. In an ex vivo design, 145 DCD renal allografts (71 AED, 74 ASED) underwent standardized hypothermic rehabilitation, with evaluations at 30, 60, and 120 min. Oxidative stress was quantified by lipid peroxidation and antioxidant capacity, in addition to histopathology (tubular, endothelial, podocyte, nuclear injury) and composite indices for cytokine activation, endothelial injury, and immune activation. A multicriteria scoring algorithm was used to categorize rehabilitation effectiveness, and group differences were assessed using comparative tests. These findings support a dynamic, multicriteria viability framework, indicating that ASED kidneys are at a higher risk yet potentially salvageable under comprehensive perfusion rehabilitation, warranting prospective transplantation-linked validation. Lipid peroxidation increased over time, rising more in the ASED group, whereas glutathione showed limited compensatory change. The ASED kidneys demonstrated greater tubular degeneration, endothelial swelling, podocyte injury, and nuclear alterations, with higher oxidative, inflammatory, and immune activation scores. Despite the higher biological burden, positive integrated outcomes remained frequent (AED 89.2% vs. ASED 84.5%; RR: 0.982; OR: 1.07–1.16), and morphology-function correlations were strong (AED r = 1.0; ASED r = 0.9). These findings support a dynamic, multicriteria viability framework, indicating that ASED kidneys are at a higher risk yet potentially salvageable under comprehensive perfusion rehabilitation, warranting prospective transplantation-linked validation.

 194 (Views)
194 (Views)  109 (Downloads)
109 (Downloads)